Genetic Profile Variation in Vaccine Strains and Clinical Isolates of Bordetella pertussis Recovered from Iranian Patients
-
Haghighi, Faezeh
-
Division of Microbiology, Department of Pathobiology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Abbasi, Ebrahim
-
Department of Bacterial Vaccines, Razi Vaccine and Serum Research Institute, Karaj, Iran
-
Eshraghi, Seyed Saeed
-
Division of Microbiology, Department of Pathobiology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Zeraati, Hojjat
-
Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Mousavi, Seyed Ali Javad
-
Department of Pulmonology, Hazrat Rasool Hospital, Iran University of Medical Sciences, Tehran, Iran
-
Asgarian-Omran, Hossein
-
Department of Immunology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Department of Immunology, School of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
-
 Douraghi, Masoumeh
Division of Microbiology, Department of Pathobiology, School of Public Health, Tehran University of Medical , Tel: +98 21 42933152; Email: mdouraghi@tums.ac.ir
Douraghi, Masoumeh
Division of Microbiology, Department of Pathobiology, School of Public Health, Tehran University of Medical , Tel: +98 21 42933152; Email: mdouraghi@tums.ac.ir
-
Division of Microbiology, Department of Pathobiology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Shokri, Fazel
Monoclonal Antibody Research Center, Avicenna Research Institute, ACECR, Tehran, Iran, Tel: +98 21 22432020; Email: fazshok@yahoo.com
-
Department of Immunology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
-
Monoclonal Antibody Research Center, Avicenna Research Institute, ACECR, Tehran, Iran
Abstract: Background: Re-emergence of pertussis has been reported in Iran despite a high rate of vaccination coverage. Low efficacy of the vaccine might be due to the genetic divergence between clinical versus vaccine strains. In the current study, the genetic profiles of clinical isolates and vaccine strains of Bordetella pertussis (B. pertussis) were assessed by using Pulsed Field Gel Electrophoresis (PFGE).
Methods: Following phenotypic and molecular identification of isolates, XbaI-digested genomic DNA of 5 clinical isolates, 2 vaccine strains and a Tohama I strain were analyzed by PFGE along with B. parapertussis as a control.
Results: Seven distinct PFGE profiles were found among all examined isolates/strains. In 5 clinical isolates, 4 profiles were identified whereas the vaccine strains displayed 2 distinct profiles. The reference strain, Tohama I had a distinct profile. Vaccine and clinical profiles had low similarity, with relatedness of approximately 40%.
Conclusion: The genetic profiles of B. pertussis were different between circulating isolates and vaccine strains used in the national vaccination programs. Since new genetic profiles of B. pertussis can be disseminated periodically, the profiles of isolates circulating in the population should be monitored over the course of the re-emergence.
Introduction :
Bordetella pertussis is a strict human pathogen causing severe contagious respiratory infection, whooping cough or pertussis 1. Pertussis remains one of the ten leading causes of death from infectious diseases among children 2. The development of whole-cell pertussis (wP) vaccines since 1950s, and the broad use of this vaccine has greatly reduced the incidence of pertussis in developed and developing countries. Despite the Expanded Program of Immunization (EPI), pertussis has not been eradicated and the re-emergence of the disease is reported worldwide 3. Re-emergence of pertussis is attributed to several factors such as waning of vaccine-induced immunity, pathogen adaptation, antigenic divergence between vaccine strains and circulating clinical isolates, and the resurgence of new variants of B. pertussis 4-6.
According to the World Health Organization (WHO) reports, the diphtheria toxoid, tetanus toxoid and pertussis (DTP) vaccine coverage is estimated to be greater than 96% in Iran since the year 2000 7. However, the pertussis cases increased from 464 in 2010 to 650 in 2011 and the national vaccination programs had a limited impact on the incidence of pertussis in various districts of the country in recent years 8. One study in assessment of the immune response against B. pertussis in Iranian children showed that half of the vaccinated children aged 8 months to 6 years did not display protective antibody levels to pertussis antigens 9. Evaluation of the immunogenicity of Diphtheria, Tetanus and whole-cell Pertussis (DTwP) vaccine used in Iran also demonstrated lower immunogenicity against pertussis compared to diphtheria and tetanus 10. Moreover, the majority of reported pertussis cases in 2009-2010 were children vaccinated by DTwP 11.
Since one reason for low efficacy of the vaccine might be the genetic divergence between vaccine and clinical strains, studies should be designed to characterize the genomic pattern of the circulating isolates and vaccine strains of B. pertussis. The aim of this study was to determine the genetic profiles of clinical isolates and vaccine strains of B. pertussis using a golden standard typing method with high discriminatory power, PFGE.
Materials and Methods :
Isolates/strains and growth condition: A total of 11 suspected clinical isolates of B. pertussis named Bp1-11 (Pertussis Reference Laboratory, Pasteur Institute of Iran, Tehran, Iran), Tohama I (ATCC® BAA-589™) as reference strain, and 2 vaccine strains (Department of Aerobic Bacterial Vaccines, Razi Vaccine and Serum Research Institute) were studied. B. parapertussis (ATCC:15311) was included as a control. Two vaccine strains used in this study were Bp509, and Bp134. These two strains have been used for production of DTwP vaccine in Iran. Two subcultures of Bp509 strain, including Bp509/1997 and Bp509/2000 were available. These isolates were prepared and frozen in 1997 and 2000 from the original stock of Bp509. Frozen bacteria were cultured onto Bordet-Gengou Agar (BGA) (Becton Dickinson, USA) supplemented with 1% glycerol, peptone, and 20% defibrinated sheep blood and were incubated at 35°C for 72 hr.
Phenotypic identification: Colonies were identified as B. pertussis by a combination of colony morphology, growth rate, Gram stain, and biochemical tests such as oxidase, catalase, urease, nitrate reductase, and lack of growth on the MacConkey and blood agar 12.
Molecular identification: Genomic DNA extraction was performed using the standard phenol-chloroform extraction method 13. Specific primers targeting insertion sequence 481 (IS481) and pertussis toxin promoter (ptxP) were used to amplify 181 base pair (bp) and 573 bp products 14,15, respectively (Table 1). Amplification of IS481 region was carried out in a total reaction volume of 20 μl containing 2 μl 10 PCR buffer (CinnaGen co., Iran), 1.5 mM MgCl2 (CinnaGen co., Iran), 0.2 mM deoxynucleotide (CinnaGen co., Iran), 0.25 mM of each primer (Bioneer, Seoul, South Korea ), 0.5 U Taq polymerase (CinnaGen co., Iran), and 10 ng DNA. The Thermocycler (Peqlab, Germany) was set with the following conditions: Initial denaturation for 5 min at 95°C and 30 cycles including denaturation for 30 s at 95°C, annealing for 30 s at 54°C, extension for 2 min at 72°C, and final extension for 10 min at 72°C. For amplification of ptxP, in a total volume of 25 μl, the same reaction mix was used as described above, with the exceptions that Taq polymerase was increased to 1 U, 10% of dimethyl sulfoxide (CinnaGen co., Iran) was added, and annealing temperature was increased to 58°C. Electrophoresis was performed in a 1% agarose (Invitrogen, USA) gel and was stained with 0.5 μg/ml ethidium bromide (Sigma, USA).
Pulsed field gel electrophoresis (PFGE): A single colony of each clinical isolate and vaccine strain confirmed as B. pertussis were subcultured onto BGA. The bacterial suspension was prepared in Cell Suspension Buffer (CSB) containing 100 mM Tris-HCl (Merck, Germany) and 100 mM EDTA (Promega, UK) with an optical density of 0.5 at 650 nm. Each plug was prepared by adding 120 μl of bacterial suspension and 20 μl of 50 mg/ml proteinase K (Sigma, USA) to 120 μl of 1% Seakem Gold agarose (FMC BioProducts, Rockland, ME) and was incubated in lysis buffer [100 mM Tris-HCl, 100 mM EDTA, 1% lauroyl sarcosine (Sigma, USA), and 0.5 mg/ml solution of proteinase K (Sigma, USA)] at 55°C overnight. The plugs were washed with deionized water and 1TE (10 mM Tris-HCl, 1 mM EDTA). The plug slices were incubated with 30 U of XbaI (Fermentas, Lithuania) at 37°C for 16 hr. PFGE was performed with 1% agarose gel in a contour-clamped homogeneous electric field (CHEF-DRIII) (Bio-Rad, USA) apparatus at 6 V/cm with a 120°C angle for 23 hr at 12°C with initial switch time of 2.2 s and the final switch of 55 s. The genomic DNA of Salmonella enterica serotype Braenderup H9812 was used as the size marker. The obtained XbaI PFGE profiles were analyzed using GelComparII version 4 (Applied Maths, Sint-Martens-Latem, Belgium). The unweighted Pair Group Method with arithmetic mean Algorithm (UPGMA) was used as the clustering method, with a 1% band tolerance, 1% optimization, and the Dice’s coefficient 16. The band pattern of each strain was confirmed visually. Isolates with a DNA band pattern differing by ≥1 band were defined as single type or distinct PFGE profile.
Results :
Isolates as small, smooth, gray colonies which appeared at a minimum of 72 hr on BGA were identified as B. pertussis and they were stained as Gram negative coccobacilli. B. pertussis colonies did not grow on common laboratory media such as MacConkey agar and blood agar and were distinguished from other Bordetella species by oxidase- and catalase-positive but urease- and nitrate-negative reactions. As indicated in table 2, five of 11 suspected clinical isolates and all vaccine strains as well as Tohama I were verified as B. pertussis based on phenotypic and biochemical characteristics.
Five of the 11 clinical isolates and all vaccine strains yielded 181 bp (Figure 1) and 573 bp (Figure 2) amplicons through amplification of IS481 and ptxP, respectively, confirming the identity of B. pertussis. A total of 5 clinical isolates, 2 vaccine strains, and Tohama I strain were firmly confirmed via both phenotypic and molecular methods. Chromosomal DNA of these confirmed strains were typed using PFGE. Seven distinct PFGE profiles were found among all examined strains. In the 5 clinical isolates, 4 profiles were identified and named C1 to C4. Two clinical isolates with the same number as well as same profiles for bands size were grouped in common type 1 (CT1). The other clinical isolates (Bp3, Bp5, and Bp9) had 80% of similarity, therefore belonged to three different types, named single type 3, 1, and 2 (ST3, ST1, and ST2), respectively. The 2 vaccine strains displayed 2 distinct profiles and were named V1 and V2. Two vaccine isolates which were derived from the Netherlands strain Bp509 had exactly the same profile and were grouped in CT2. The vaccine strain, Bp134, had unique PFGE profile and was defined as ST5. As shown in figure 3, Tohama I strain was included in dendrogram as a reference strain (R1) with unique profile and was considered as ST4. Vaccine profiles and clinical profiles had low similarity, with relatedness of approximately 40%. B. parapertussis which was used as a control had distinct PFGE profile with low relatedness (<40%) to all typed B. pertussis isolates/strains.
Discussion :
In this study, the genetic profiles of a limited number of B. pertussis isolates recovered from Iranian patients were analyzed and compared with the two strains which were used for production of the national whole-cell pertussis vaccine. PFGE as a typing method was used and different PFGE patterns among the clinical isolates were found. This finding indicated that different B. pertussis isolates were circulating despite high vaccination coverage in Iran. However, low heterogeneity has been found among the clinical isolates and these isolates belonged to different profiles with an approximately 80% of genetic relatedness. Therefore, the results were consistent with previous studies that classified B. pertussis as a genetically monomorphic pathogen 17,18.
Two strains containing the same PFGE pattern were also identified among clinical isolates. They were more likely to be related and to have a common source. Two PFGE patterns among the vaccine strains were observed in this study. These 2 profiles belonged to strains used in vaccine production in Iran. Two isolates included in V1 profile were subcultures or derivatives of a vaccine strain of the Netherlands origin, Bp509, which were cultured at different time intervals. The exactly similar PFGE patterns of our vaccine strains suggest that repeated subculture did not lead to genetic divergence over time, as previously described by Advani et al 19. However, two studies showed that the PFGE profiles changed upon repeated subculture 20,21. The XbaI digested DNA of the reference strain (Tohama I) had PFGE profile exactly similar to profile obtained by others who clustered Tohama I in PFGE group II 22. The DNA of vaccine strains Bp509 and Bp134 were also digested with XbaI and the profiles were comparable with that of other studies. The strain Bp509 showed exactly similar profile same as several other studies 23-25, but a controversy was found in just one study in which Bp509 and Bp134 were considered the same 23. In this study, strain Bp134 showed the same profile as reported in previous studies 26,27, but Bottero et al reported similar profiles for Bp509 and Bp134 in their dendrogram 23. This controversy may be due to an error in processing the stocks of bacteria or interpretation of the dendrogram.
Comparison of the genetic profiles of vaccine strains and clinical isolates demonstrated that vaccine strains had different PFGE patterns and were not matched to circulating isolates. One explanation for this variation might be associated to the low efficacy of currently used vaccine which may lead to adaptation of the pathogen and selection of new variants of B. pertussis 5. Another explanation is that the circulating bacteria may evade the host responses and in turn evolve efficient mechanisms to overcome the vaccine-induced immunity 28,29. It is also possible that such gross genetic variations might not be clinically relevant and reflect random mutations introduced in the genome of Bp isolates obtained from the patients. However, more detailed genetic and structural investigations are required to address this issue.
Several studies have compared the PFGE profiles of clinical isolates and vaccine strains of B. pertussis in different countries. The majority of these studies have indicated that non-vaccine isolates were recovered from patients with pertussis disease and these isolates were genetically different from the vaccine strains 19,22,30. However, in the study of Elomaa et al, the profile of one of the two assessed vaccine strains was detected among the circulating isolates 31.
Conclusion :
It was demonstrated that non-vaccine isolates of B. pertussis were different from vaccine strains used in the national vaccination program. Since new genetic profiles of B. pertussis can be disseminated periodically, the profiles of isolates circulating in the population should be monitored over the course of the re-emergence. PFGE is used as a golden standard method for determining the gross polymorphisms within restriction enzyme Recognition Sites (RS) in whole genome and for identifying the extensive rearrangements, deletions, and insertions that affect the restriction fragment profile 32. However, some genetic variations such as single nucleotide polymorphism, short tandem repeat polymorphism, non-RS repetitive sequence polymorphisms, and mutations changing the genetic code could not be assessed via PFGE. Therefore, sequencing based methods need to be used to characterize and interpret such minute and small-scale changes. Further monitoring may provide more information about the strains or antigens needed for development of more effective vaccines.
Acknowledgement :
This research has been supported in part by Tehran University of Medical Sciences and Health Services grants.
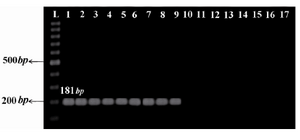
Figure 1. The IS481 amplification using specific primers yielded a product of 181 bp typical to clinical isolates and vaccine strains of B. pertussis. L: 100 bp ladder (Fermentas, Lithuania); 1: Tohama I strain as reference strain; 2-6: clinical isolates of B. pertussis; 7-9: vaccine strains of B. pertussis; 10-15: non-B. pertussis clinical isolates; 16: B. paraper-tussis; 17: Negative control (distilled water)
|
Figure 2. The ptxP amplification using specific primers yielded a product of 573 bp typical to clinical isolates and vaccine strains of B. pertussis. L: 100 bp ladder (Fermentas, Lithuania); 1: Tohama I strain as reference strain; 2-6: clinical isolates of B. pertussis; 7-9: vaccine strains of B. pertussis; 10-15: non-B. pertussis clinical isolates; 16: B. paraper-tussis; 17: negative control (distilled water)
|
Figure 3. Genomic analysis of B. pertussis using PFGE. The dendrogram shows PFGE profiles of clinical isolates (C), vaccine strains (V), and reference strain Tohama I (R1).
B. parapertussis (Bpp) was used as a control. The PFGE clusters are indicated as common type (CT) or single type (ST)
|

Table 1. Specific primers sequences targeting IS481 and ptxP
|
Table 2. Differential characteristics of vaccine strains, clinical isolates, and reference strains of B. pertussis and B. parapertussis
* Growth rate represents minimum days of appearance of colonies on BGA; Bp: Bordetella pertussis, V: Variable growth patterns
|
|