Transmitted Drug Resistance Against Integrase Strand Transfer Inhibitors in Iranian HIV-Infected Naïve Patients
-
Hashempour, Ava
-
Shiraz HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
-
Musavi , Zahra
-
Shiraz HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
-
Moayedi, Javad
-
Shiraz HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
-
Hasanshahi, Zahra
-
Shiraz HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
-
 Dehghani , Behzad
Shiraz HIV/AIDS Research Cen-ter, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran, Tel/Fax: +98 71 37386272; E-mail: dehghanibehzad@gmail.com
Dehghani , Behzad
Shiraz HIV/AIDS Research Cen-ter, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran, Tel/Fax: +98 71 37386272; E-mail: dehghanibehzad@gmail.com
-
Ghasabi, Farzaneh
-
Shiraz HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
-
Joulaei, Hassan
Shiraz HIV/AIDS Research Cen-ter, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran, Tel/Fax: +98 71 37386272; E-mail: joulaee@sums.ac.ir
Abstract: Background: Human Immunodeficiency Virus (HIV) has claimed the lives of millions of people during the past decades. While several antiretroviral drugs like Integrase Strand Transfer Inhibitors (INSTIs) have been introduced to control HIV, Transmitted Drug Resistance (TDR) in HIV genome caused failure in treatment. This study aimed to investigate TDR and natural occurring mutations (NOPs) in HIV integrase gene in Irani-an HIV patients.
Methods: In this cross-sectional study, blood samples of 30 HIV-positive patients who had never taken integrase inhibitors were considered for CD4 T cell count, RT real-time PCR, and, Nested PCR. The sequencing results were analyzed by CLC sequence viewer software and Stanford University HIV Drug Resistance Database.
Results: In all samples, nine NOPs with a high prevalence were found; however, we did not find any drug resistance mutations, except for a mutation in one sample, which showed a low resistance level. Subtype A1 was dominant in all samples.
Conclusion: Based on the findings and compared to our previous study, all patients were sustainable to main integrase inhibitors, including bictegravir, raltegravir, bicte-gravir, elvitegravir and dolutegravir. It seems the resistant mutation pattern attributed to integrase inhibitors was not diffent among studied patients; hence, the prescription of such inhibitors helps physicians to control HIV infection in Iranian HIV-infected pa-tients.
Introduction :
Acquired Immune Deficiency Syndrome (AIDS) needs intensive care support to improve the life expectancy of HIV-infected patients using Highly Active Antiretroviral Therapy (HAART) 1. One of the most important steps in the life cycle of HIV is the integration stage of the virus genome into the host genome. Regarding the critical role of the integrase enzyme in the replication of HIV, researchers have considered this protein as one of the antiviral treatment targets; therefore, several inhibitors have been considered to suppress this enzyme. Although the impact of Integrase Strand Transfer Inhibitors (INSTIs) on the activity of this enzyme is significant, the efficiency of such inhibitors has decreased with the advent of resistant treatment strains. Several factors have been proposed to emerge resistance, among which mutations in the integrase gene play a major role.
Since INSTIs are currently prescribed in Iranian patients who do not respond to other Antiretroviral Therapy (ART), several studies on Transmitted Drug Resistance (TDR) and natural occurring mutations (NOPs) of INSTIs is required to guide the implementation of such inhibitors across the country. According to the preceding issues, this study aimed to evaluate the TDR and NOPs in HIV integrase gene and also find the dominant subtype in Iranian patients.
Materials and Methods :
Ethics: All the subjects were provided written informed consent in accordance with the declaration of Helsinki and its later amendment. The research protocol was approved by the local Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (Certificate Reference Number of REC 1396.S690), and patient privacy was ensured.
Patients and samples: From January to February 2022, thirty adult Iranian patients with a confirmed history of Human Immunodeficiency Virus (HIV) who had routinely visited Behavioral Diseases Consultation Center affiliated with Shiraz University of Medical Sciences, were recruited in this cross-sectional study. The inclusion criteria were expanded to older than 18 years of age, CD4+T cell counts >200/µl, without previous exposure to ARTs. Individuals diagnosed with tuberculosis were excluded from this study. Peripheral blood samples (5 ml) were collected in non-heparinized tubes and allowed to clot. Afterward, the tubes were centrifuged at 3000 RPM for 5 min, and the serum fraction was separated, coded, and stored at -70°C until further use.
CD4 T-cell count: The number of CD4 T-cells in sera of HIV-infected patients was counted using FACSPresto Near-Patient CD4 Counter (BD Biosciences, America).
RNA extraction and real-time PCR assay: Whole RNA was extracted by the QIAamp Viral RNA Mini Extraction Kit (Qiagen, Germany), according to the manufacturer's recommendation. HIV viral load was determined in all samples using an Artus HI Virus-1 RT-PCR kit (Qiagen, Germany).
Reverse transcriptase-nested PCR assay: A sensitive and reliable RT-nested PCR assay for amplification of HIV-INT region was performed using the primers 2 listed in table 1. GAPDH was chosen as Internal Control (IC).
Sequencing: The positive PCR amplicons were purified by a gel extraction kit (QiagenGmbH, Hilden, Germany), according to the manufacturer's protocol. Both DNA strands were subjected to Sanger sequencing with a detection limit of ~15-20%. (Niagene Noor Company, Iran). The sequences were examined using the CLC sequence viewer software, and the mutations were determined in comparison with the reference sequences with the accession number AB703607. Subtypes of HIV and TDR and NOPs in integrase genes were determined in all samples via the Stanford University HIV Drug Resistance Database site.
Results :
The results showed a large number of mutations in the studied samples with a relatively high frequency in several regions (Table 2). Comparison of the sample sequences with reference sequence revealed different mutations with the frequency of less than 5 to 46% in integrase genes of patients. A shown in table 2, the percentages of nine high prevalent mutations varied from 26 to 46; however, the mutations 113, 123, 136, and 127 with an incidence of 46% were considered as the highest frequent mutations. Besides, the analysis suggested that in all samples, at least there was one of the mentioned mutations. However, only in one patient (sample 12), serine was replaced by phenylalanine due to a mutation in amino acid 153 in this region; therefore, low resistance mutation was observed for the integrase inhibitors. Furthermore, the subtyping analysis showed that all samples belonged to subtype A.
Discussion :
Different studies used bioinformatics tools to describe mutations 3,4. In the present research conducted on HIV-infected patients who had not received integrase inhibitors, all mutations in HIV integrase gene was investigated using bioinformatics software. The results from thirty Iranian patients represented nine amino acid changes with high frequency. Analysis of the patients' sequences revealed the presence of three mutations with a frequency of about 46%, which provided a higher frequency compared to similar studies. The present investigation indicated that all enrolled patients had at least one of 9 examined mutations in the sequenced region.
Similar to our previous study, as the most recent study on the integrase gene in Iranian patients from 2017 to 2020, HIV drug resistance mutations did not affect the drug susceptibility to integrase inhibitors. In agreement with our data, Jahanbakhsh et al 5 and Farrokhi et al 6 did not identify any drug resistance mutations in the integrase gene of Iranian patients. However, four mutations, including T66A, Y143R, Y143R, and T97A were introduced as resistance mutations in another study that presented moderate to high resistance levels to related inhibitors 7, but none of them were found in the current study.
In reports from other countries, multiple mutations have suggested HIV integrase gene as drug-resistance mutations. Among them, mutations in amino acids 118, 263, 66, and 92 have been identified as major drug-resistance mutations, none of which have been found in this study 8-10. The difference between the present and previous findings may be due to moderate changes in the virus genome, geographical location, and sample size.
Given that in the present study, the reported mutations did not lead to drug resistance to integrase inhibitors, it seems integrase inhibitors should be prescribed along with the current regimen for Iranian patients. In the present data, A1 was the dominant subtype in patients, and there was no significant relationship between viral load, sex, and gender with resistance mutations. Subtype A1 reported here was similar to previous studies 11-13. In contrast to our findings, subtype AD has been introduced as the main subtype of Iranian patients in several studies. Baesi et al 14-16 also reported different subtypes, including A1, B, and CRF35 AD. The differences can be due to analyses of various genome regions, subtyping tools, and the introduction of new mild diversity Iranian HIV subtypes in recent years.
Conclusion :
Generally speaking, this study showed no significant mutations concerning the resistance to integrase inhibitors in Iranian HIV-infected patients. Using such inhibitors in the treatment of Iranian patients increases the chances of responding to treatment in patients with HIV, which can reduce the transmission rate of the virus in the community and thus can be taken to achieve the goals of the 90-90-90 plan. Moreover, the present finding indicated the importance of HIV subtyping among Iranian patients; the results can predict the transmission route and the plausible level of virus pathogenicity.
Acknowledgement :
This study was funded by Shiraz University of Medical Sciences (grant number: 1396-01-59-15180). The authors would like to thank Dr. Nasrin Shokrpour for the editorial assistance.
Conflict of Interest :
The authors declare no conflict of interest.
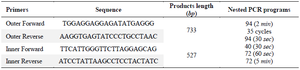
Table 1. List of primers used in this study and thermal-cycling conditions of nested-PCR assay
|
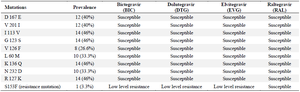
Table 2. The mutations found in the sample compared with the reference sequence
|
|