Effects of Sperm Chromatin Integrity on Fertilization Rate and Embryo Quality Following Intracytoplasmic Sperm Injection
-
Sadeghi, Mohammad Reza
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Hodjat, Mahshid
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Lakpour, Niknam
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Arefi, Soheila
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Amirjannati, Naser
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Modarresi, Tahereh
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
Hossaini Jadda, Hossain
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
-
 Akhondi, Mohammad Mehdi
Ph.D., Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran, P.O. Box: 19615-1177, Tel: +98 21 22432020, Fax: +98 21 22432021, E-mail: akhondi@avicenna.ac.ir
Akhondi, Mohammad Mehdi
Ph.D., Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran, P.O. Box: 19615-1177, Tel: +98 21 22432020, Fax: +98 21 22432021, E-mail: akhondi@avicenna.ac.ir
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR , Tehran, Iran
Abstract: Sperm chromatin integrity has been being recognized as an important factor in male fertility. During normal fertilization, high quality sperm with intact chromatin are selected through natural selection in journey from vagina to fallopian tube. However, using Assisted Reproductive Techniques, particularly ICSI, the natural selection is bypassed. Therefore sperm with DNA breakage have the opportunity to fertilize the egg which may lead to decreased embryo quality and implantation rate. The aim of this study was to evaluate the effects of sperm chromatin integrity on ICSI outcomes. A total of 200 semen samples were collected from couples undergoing ICSI and were analyzed according to WHO criteria. Each sample was evaluated for sperm chromatin integrity using four cytochemical assays and semen processing by swim up method. The ICSI was carried out according to a long-term pituitary down-regulation protocol. The correlation between sperm parameters, sperm chromatin integrity and ICSI outcomes (fertilization rate and embryo quality) was examined. The mean number of oocyte, fertilization rate and cleavage embryos per cycles was 7.5±5.0, 74.06%±25 and 5.4±3.6, respectively. There was not significant correlation between the results of chromatin assays (AO, AB, TB, and CMA3) and fertilization outcomes following ICSI. The fertilization rate was significantly higher for a group with less than 10% chromatin abnormality (p<0.05). Sperm chromatin integrity is essential for successful fertilization, embryo development and normal pregnancy. A protamine deficiency appeared to affect fertilization rate and embryo quality. However, the presence of confounding factors such as selection of spermatozoa according to normal morphology may influence the effect of sperm chromatin status on ICSI outcomes.
Introduction :
The field of Assisted Reproductive Tech-nology (ART) including ICSI, IVF and IUI has been significantly developed in the last two decades and consequently demand for such treatments have dramatically increased. In Europe, the number of ART treatment is more than 270,000 per year (1) and in United state the number of ART treatment
cycles rose from approximately 59,142 cycles in 1995 to 115,392 cycles in 2002 (2).
Among various assisted reproductive tech-niques, ICSI has become a preferred and widely applied method for helping infertile couples to achieve conception (3,4). There is also an increased tendency for ICSI than IVF, according to Human Fertilization and Embry-ology Association (HFEA) statistics (5). How-ever, despite the incredible success and broad use of ICSI, these techniques carry some risks. It is argued that through bypassing the natural selection of sperm-zona penetration, the risk of oocyte fertilization by defective sperm will be increased which then can lead to malformations in the offspring (6). During ICSI, the embryologist attempts to select the best spermatozoa according to its morphology and motility as markers of normality and via-bility. However, according to the recent studies the routine sperm analyses such as sperm count, motility and morphology, are not reliable indicators of sperm function and chromatin integrity (7,8). Therefore sperm with normal motility and morphology, but con-taining chromatin abnormality will be given the chance to penetrate and fertilize the eggs.
Sperm functional assay is considered as the valuable diagnostic tool in evaluation and pre-diction of male infertility (9-13). Different studies have assessed the diagnostic potential of this assay in the outcome of assisted repro-ductive technologies (ART). Sperm chromatin is tightly packaged to protect DNA during the transit that occurs before fertilization. Any ab-normality in chromatin structure and integrity could lead to failure in fertilization. A variety of tests have been described to assess sperm chromatin status that are considered as valu-able predictive tools for in vivo and in vitro fertilization outcomes. However, there were widespread controversies over the relation-ships between sperm chromatin status and ICSI outcomes. Based on various studies of different cases subjected to ICSI program, ab-normal sperm factors lead to low fertilization rate and poor embryo quality (14-17). In contrast there are studies indicating that fertilization rate, embryo cleavage and pregnancy rates are independent of sperm parameter in ICSI (18). To further assess the importance of semen routine parameters and sperm chromatin integrity on ICSI outcomes, we conducted an experimental study to determine the relation-ship between sperm chromatin status using four cytochemical staining assays [Chromo-mycin A3 (CMA3) for protamine deficiency, Aniline Blue (AB) for abnormal persistence of histones, Toluidine Blue (TB) and Acridine Orange (AO) for DNA abnormality] and ART results (fertilization rate, cleavage rate and embryo quality) during the ICSI treatment.
Materials and Methods :
A total of 200 semen samples were collect-ed from couples undergoing ICSI at Avicenna Infertility Clinic (AIC), Tehran, Iran. The in-formed written consent for use of the surplus semen in this research was obtained from the couples in accordance with the Avicenna Research Institute Medical Ethics regulation in research involving the human subjects. The cryopreserved semen samples and also sam-ples with less than 1×106 sperm/ml were ex-cluded from the study. The inclusion criteria for the female partner was age <35 yrs.
Semen collection and preparation
Briefly, on the day of oocyte aspiration, semen sample was produced on-site by mas-turbation and allowed to liquefy at 37°C for 20 min prior to analysis. Each sample was divided in two aliquots to be used for analysis of sperm parameters and another part was used for sperm processing to inseminate oocytes via ICSI. The sperm parameters of counts, motility and morphology were ana-lyzed according to WHO guidelines using raw semen sample (19). Swim up processing was performed as previously described (20).
ART procedure
The Controlled Ovarian Hyperstimulation (COH) was performed according to the long luteal suppression protocol, using a GnRHa (Superfact, Ferring, Germany) and combin-ation of HMG (Menogon, Ferring, Germany) or recombinant FSH (Gonal-F, Serono, Swit-zerland). The ovulation was induced when at least three follicles had a diameter of =18 mm, using 10,000 IU HCG (Choriomon, IBSA, Switzerland). Transvaginal oocyte retrieval was performed by ultrasound guidance. The oocytes containing cumulous cells were col-lected from clear follicular fluid. Granulosa cells were separated from collected oocytes using enzymatic (Collagenase, Sigma) and mechanical digestion. The ICSI was per-formed as previously described (21). Luteal phase support was performed using intra-vaginal and intramuscular progesterone ad-ministration (Osveh, Iran).
Embryos
The oocytes were assessed for fertilization at 16-18 hrs after microinjection (two pro-nuclear stage, 2PN). The embryos were graded according to their morphology, 48 hrs after insemination. The classification was as follows: grade A: no fragmentation and four regular cells; grade B: <25% fragmentation; grade C: between 25 and 50% fragmentation and grade D: >50% fragmentation (22). The transfer of the embryos took place either at 48 or 72 hrs after the ICSI, according to the treatment plan of the center.
Acridine Orange staining (AO)
The method for Acridine Orange staining was the modified protocol previously de-scribed (23,24). A raw semen sample was wash-ed three times in Phosphate Buffered Saline (PBS). Thick smears of washed spermatozoa were prepared on pre-cleaned degreased slides (product: 7201, Surwin Plastic Enter-prises, China) and allowed to air-dry for 10min. The smears were fixed for 1hr in ethanol-acetone (1:1) at 4°C and allowed to dry for a few minutes before staining for
7 min with AO (0.19 mg/ml) at room tempera-ture. The AO staining solution was prepared as follows: 10 ml of 0.1% AO stock solution in distilled water was added to a mixture of
40 ml of 0.1 M citric acid and 2.5 ml of 0.3 M Na2HPO4.7H2O, pH=2.5. After staining, the slides were gently rinsed in a stream of distil-led water and air dried. This was followed by evaluation under fluorescence microscope (Zeiss, Germany) with a 100×oil immersion objective. Sperm heads with intact chromatin had green fluorescence, and those with dena-tured chromatin had orange-red staining. Each sample was scored within 1 hr after staining. At least 200 sperm per slide were evaluated to estimate the number of sperm stained with green and red fluorescence.
Toluidine Blue staining (TB)
The air-dried smears were fixed according to AO staining and allowed to dry for a few minutes before staining with 0.05% Toluidine Blue (Merck, Germany) in staining buffer for 10 min. The staining buffer consisted of 50% citrate phosphate (McIlvain buffer, pH=3.5) (25). After stainin
Result :
For this study, 200 semen samples were collected. A sample of 28 were excluded from the study due to insufficient volume of semen sample, lack of oocyte retrieval following puncture and due to anomalies and low qual-ity of oocytes. The mean age of male partici-pant was 33.9±6 years. The results of semen analysis, chromatin assay and the ICSI cycle results are summarized in Tables 1 and 2. According to results of semen analysis, there were 64 (37.2%) normozoospermia, 12(7%) oligoasthenoteratozoospermia, 48 (27.9%) as-thenoteratozoospermia, 44 (25.6%) teratozoo-spermia, 3 (1.7%) astenozoospermia, and 1 (0.6%) oligozoospermia. The mean age of female participant was 30.2±5 yrs.
Semen parameters and fertilization rate
The mean fertilization rate was 74.06±25 and there were no significant correlations be-tween sperm function tests and fertilization rate. However, when chromatin integrity was measured by aniline blue divided in two groups according to a threshold of 10%, the fertilization rate was significantly higher for the group with less than 10% chromatin ab-normality (85±22.3 vs. 73.4±25.4) (p<0.05). However this was not significant for grouping according to thresholds of 20% or 30%. Also, the fertilization rate following ICSI was not influenced by sperm parameters of motility, morphology and concentration (p>0.05) (Table 2). Grouping was according to the previously studied threshold for chromatin assays (28).
Sperm chromatin integrity and embryo quality
The average percentage of embryo quality (grade A, B, C) is summarized in Table 2. When cases were divided according to the threshold of 30% abnormal chromatin using Chromomycin A3 (29,30), a significant differ-nce was observed for embryo quality (grade A) between the two groups (p<0.05). The em-ryo quality grade A was 71.3% when CMA3 results were less than 30% and 57.2% when CMA3 results were greater than 30%. There were significant negative correlations be-ween embryo quality grades A, B and per-entage of abnormal chromatin using CMA3 staining (Table 3).
Discussion :
In the present study, four different cyto-hemical staining methods including Toluidine Blue, Aniline Blue, Chromomycin A3 and Acridine Orange assays were applied in order to assess different aspects of sperm DNA integrity (31). The Chromomycin A3 (CMA3) staining was applied for the evaluation of protamine deficiency, Aniline Blue staining to detect excessive presence of histones; Tolui-dine Blue and fluorescence Acridine Orange, as a sensitive structural probes, were used for assessing sperm chromatin structure and packaging (23,32,33). The TB is a classic nuclear dye used for external metachromatic and orthochromatic staining of chromatin, which overall is negatively charged (23,25). It becomes heavily incorporated in damaged dense chro-matin and can be used as a fairly reliable method for assessing the integrity of sperm chromatin. The AO assay measures the sus-ceptibility of sperm nuclear chromatin to acid induced denaturation in situ by quantifying the metachromatic shift of AO fluorescence from green (native chromatin) to red (dena-tured chromatin). This stain is a sensitive structural probe for chromatin structure and packaging, assessed either by microscopy or flow cytometry.
Our results showed that when the cases were divided in two groups according to chro-matin abnormality, fertilization rates were significantly increased in the group with less than 10% abnormal chromatin threshold using Aniline Blue. Such finding may indicate that protamine deficiency has considerable affect on fertilization rate. However in case of grouping by 20% or 30% thresholds of abnor-mal chromatin, no significant differences were found between the two groups. We also found no significant correlation between other chromatin staining assays and fertilization rate. This was in agreement with Sakass and Zini (34,35) that found no significant correlation between Chromomycin A3, Acridine Orange and Toluidine Blue with fertilization rate in infertile couples undergoing IVF/ ICSI. Also, our results were in agreement with the finding of Hammadeh and his colleagues, that re-ported no significant correlation between sperm with abnormal chromatin and fertil-ization rate and embryo quality with regard to 30% cut off for DNA fragmentation using Aniline Blue staining (27). In contrast, there are broader studies showing negative associations between frequency of sperm DNA fragmenta-tion and fertilization rate and embryo devel-opment (36-39). Therefore, there are still contro-versies over the affect of sperm chromatin status on fertilization rate and pregnancy out comes (40).
Normal sperm chromatin structure and integrity is essential for the accurate trans-mission of paternal genetic information to the next generation and also appropriate function of sperm in the fertilization process (41,42). It has been shown that sperm with protamine deficiency and increased histone remnants, lead to premature chromatin condensation that is the cause of failures in fertilization and embryo development (43-45). Moreover, the chromatin of sperm with reduced amounts of protamine was observed to be susceptible to chemical disruption (46). Considering all these studies, it is most probable that sperm with abnormal chromatin can affect fertilization rate and embryo quality following ICSI procedure.
A reason for the current findings of "no significant correlation between fertilization rates and most of the sperm parameters" may be due to the fact that assays for sperm chro-matin abnormalities were performed on raw semen samples that contained large numbers of immotile, nonviable or degenerated sperm with abnormal chromatin. However, through pre-ICSI processing techniques (gradient cen-trifugation, swim up or glass wool, etc.) most abnormal sperms are removed and the result-ant processed semen contain motile sperm with normal morphology (47-49). Because that such processed sperm possess greater quality, assessment of the correlation between sperm parameters in raw semen samp
Acknowledgement :
The authors would like to thank Dr H. Zeraati for assistance with statistical analyses and S. Behnam Hashemi (MD, MPH) for kindly editing the article.
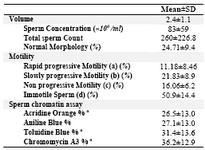
Table 1. Summery of semen analysis and sperm chromatin assay results in 172 men undergoing ICSI treatment a Percentage of sperm with abnormal chromatin
|
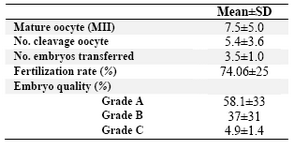
Table 2. Summary of embryology results in 172 couples undergoing ICSI cycle
|
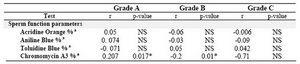
Table 3. Correlation between sperm function test results and embryo quality
* p<0.05, a: Percentage of sperm with abnormal chromatin, NS= not statistically significant; r = Pearson�s correlation coefficient
|
|