High Prevalence of Y Chromosome Partial Microdeletions in Overweight Men
-
 Golalipour, Masoud
Department of Biology, School of Basic Sciences, Golestan University, Gorgan, Iran, Tel: +98 171 2245964, E-mail: m.golalipour@gu.ac.ir
Golalipour, Masoud
Department of Biology, School of Basic Sciences, Golestan University, Gorgan, Iran, Tel: +98 171 2245964, E-mail: m.golalipour@gu.ac.ir
-
Department of Biology, School of Basic Sciences, Golestan University, Gorgan, Iran
-
Hadadchi, Gholamreza
-
Department of Biology, School of Basic Sciences, Golestan University, Gorgan, Iran
Abstract: Background: Microdeletions of the Y chromosome are one of the most frequent genetic causes of spermatogenic failure in infertile men. But their role in gaining weight is unclear. The present study investigated the possible association of these partial microdeletions and obesity.
Methods: In a case-control study, 180 males were selected. The prevalence of microdeletions was assessed using PCR in AZFc area of Y chromosome and statistical analysis was done using the Fisher exact test and Pearson correlation.
Results: In our study, inverse relationship was observed between body mass index and testosterone level (p-value: 0.005). Fisher exact tests showed that there was a significant association between gr/gr mutation and BMI (p-value: 0.044).
Conclusion: Our study revealed that Y chromosome microdeletions are more common in obese men. Furthermore, microdeletions such as gr/gr, which were observed in normal men, could cause decreased testosterone level. So, they may contribute to gaining weight.
Introduction :
The absolute number of obese individuals is estimated to be totally 2.16 billion ones and 1.12 billion by the year 2030 1. So, it's important to find the most common causes of this major challenge. Obesity results from combination of environmental and genetic factors 2. Despite extensive studies on the genes involved in obesity, the Y chromosome genes are largely ignored. Even in studies of genome-wide scans, the Y chromosome is excluded 3.
MSY region on the Y chromosome is divided into three parts: AZFa, AZFb, and AZFc 4. The AZFc region has 12 genes. Complete removal of this region, which eliminates 5.3 Mb, is the most common pattern among infertile men with Y chromosome deletions. In addition, partial microdeletions such as gr/gr or b1/b3 exist in this region 5-7. Partial microdeletions are seen in both infertile and normal men and their role is unclear in fertility 8.
Partial microdeletions remove parts of the AZF region with no significant impact on fertility, but they may have side effects such as decreased androgen level and increased BMI. In this study, the association between obesity and partial microdeletions of the Y chromosome was investigated.
Materials and Methods :
Study population: A case-control study was performed with 180 participants from Golestan Province (138 cases and 42 controls). The data were collected from 2011 to 2012. Ten to eighty year old men were selected. Samples younger or older than this age range were excluded. The study protocol was approved by the Ethics Committee of the Golestan University (Golestan, Iran) and informed consent was collected from participants prior to recruitment.
Anthropometric measurements: Using a digital scale, participants' weight was measured with a precision of 0.1 kg. Height was measured in centimeter with an accuracy of a decimal point. The body mass index calculated as weight in kilograms was divided by the square of the height in meters (kg/m2) 9. The subjects were divided into three categories according to Body Mass Index (BMI) 10: Normal weight (18.5<BMI≤24.9), overweight (25<BMI≤30) and obese (BMI>30). Testosterone level was measured using ELISA kits (Monobind). Next, 2.5 ml of blood was stored in a refrigerator at 4°C for molecular assay.
Genotyping: Genomic DNA was extracted using standard phenol-chloroform method. Samples were centrifuged at 3000 RPM for 10 min at room temperature within 1 hr of collection. Plasma and red blood cells were separated and stored at 70°C. Amplification of the AZF region of the Y chromosome was performed using forward and reverse primers (Table 1).
To figure the AZF microdeletions, first PCR was conducted in two multiplexes:
Multiplex A: ZFY: 495 bp, sY84: 326 bp (AZFa), sY134: 301 bp (AZFb), sY255: 126 bp (AZFc)
Multiplex B: SRY: 472 bp, sY254: 400 bp (AZFc), sY86: 320 bp (AZFa), sY127: 274 bp (AZFb)
PCR was carried out in 25 µl reaction volume containing each primer 1 μM, 2.5 μM enzyme buffer, 2 μM Mgcl2, 1 μM dNTP mix and, 0.2 μM Tag enzyme. Then, the extracted DNA was added to 1 μM in 25 μl total volume (all materials from TaKaRa, Seoul, Korea). Reactions were amplified by these steps: initial denaturation at 94°C for 5 min, followed by 30 cycles of denaturation at 94°C for 20 s, annealing at 57°C for 5 min, extension at 72°C for 45 s, followed by a final extension at 72°C for 5 min. PCR products were separated by electrophoresis on a 1.5% agarose gel and visualized by staining with ethidium bromide under ultraviolet light.
After determining the AZF deletions, samples with complete AZF deletion were discarded and individuals who did not carry AZF microdeletions were screened for partial AZFc microdeletions. Each individual was screened with two STSs specific for the gr/gr region, sY1291 and sY1191.
The second amplification program included an initial denaturation step at 94°C for 5 min, amplification for 30 sequential cycles, each including 30 s denaturation at 94°C, 30 s annealing at 51°C and 1 min extension at 72°C and a final extension step at 72°C for 5 min.
Statistical analysis: The Kolmogorov-Smirnov test was used to test the normality of the data. Data were expressed as mean±standard deviation (SD). To compare the results, Fisher exact tests and the Pearson correlation were used. SPSS (SPSS version 16, SPSS Inc., Chicago, USA) was used for data analysis. A p-value of 0.05 was considered as the threshold significance level for each test.
Results :
One hundred and eighty subjects were screened for Yq microdeletions. The study population comprised 44 obese, 94 overweight and 42 normal men. Clinical and anthropometric parameters were determined (Table 2).
The Pearson correlation was used to compare testosterone level with BMI. A significant relationship was observed between this hormone and BMI (p-value: 0.005). Samples with lower testosterone levels were obese or overweight.
PCR was performed with eight pairs of primers for all samples (Figure 1). Samples which had a complete mirodeletion were discarded (Table 3). To find partial microdeletions, PCR was conducted with sY1191 and sY1291 primers on the rest of the samples (Figures 2 and 3).
In the study, 8 overweight and 5 obese men carrying the gr/gr deletion (13/150, 9.3%) were recognized. Two cases with b2/b3 deletion were observed in the normal population, and in overweight and obese groups, 5 and 2 cases were detected with b2/b3 deletion, respectively. Only one case with b1/b3 deletion was found in the obese group (Table 4).
Fisher exact tests showed that there was a significant association between gr/gr mutation and BMI (p-value: 0.044, OR 0.27, 95% CI 0.03-2.18). But b1/b3 and b2/b3 deletions showed no significant correlation to BMI (Table 5).
Discussion :
This study demonstrated that the Y chromosome microdeletions are more common in obese men. Also, with increasing age and BMI in men, testosterone levels decline. Epidemiologic studies have shown that a bidirectional relation exists between obesity and testosterone level 11-13. Because of such relationship between weight gain and testosterone level, administration of this hormone for losing weight in men is considered as a therapeutic approach 14,15. Excess aromatase activity in adipose tissue could decrease testosterone and increase estrogen level 11. Some studies demonstrate that aromatase inhibition is an effective means in increasing testosterone production in elderly men with low or borderline low serum testosterone levels 16,17.
From the past, the role of AZF region in infertility is always emphasized 8. But in this study, regardless of Y chromosome microdeletions’ role in infertility, their association with weight gain and obesity was investigated. One of the most common deletions in the AZF region is a complete AZFc deletion which leads to infertility. The complete removal of this region deletes all DAZ (deleted in azoospermia) gene copies and 21 other transcription units. Consequently, it may decrease testosterone level which leads to an increase in BMI. Smaller deletions, such as gr/gr, exist in AZF area, known as partial microdeletions. Partial microdeletions are found in infertile and fertile men as well. So, their role in infertility still remains controversial. The present study shows a significant association between gr/gr deletion and BMI. It seems that overweight men have a higher incidence of partial microdeletions compared to normal men.
Conclusion :
In conclusion, besides complete AZFc deletions, partial microdeletions such as gr/gr have also occurred in men. These partial microdeletions may exert effects which lead to low levels of testosterone. Our study showed that partial AZFc deletions could increase the risk of obesity in men. Long term studies are needed to assess the overall consequences of these Y chromosome microdeletions in obese men.
Acknowledgement :
We thank Dr Sepehri (Sepehr Laboratory, Golestan, Iran) and Abbas Gharib for providing samples for our study. The authors thank Maryam Mardannik, Razieh Ardameh for their support. We appreciate all the DNA donors and patients without whom this work would not have been possible.
Conflict of Interest :
The authors declare that there is no conflict of interests.

Figure 1. Multiplex PCR, first lane is a 100 bp DNA ladder. Lane 1 doesn't have any deletion. Lane 2 has sY84 deletion and lane 3 has sY134 deletion.
|

Figure 2. PCR by sY1191 primer. Number 3 and 5 samples have b2/b3 deletion.
|

Figure 3. PCR by sY1291 primer. Sample number 7 has a gr/gr deletion
|

Table 1. The appendix sequence of PCR primers
|
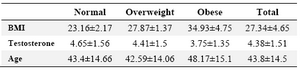
Table 2. Clinical and anthropometric variables in study groups
|
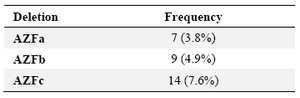
Table 3. Frequency of Y chromosome microdeletion (in AZF regions) in study population
|
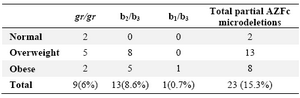
Table 4. Frequency of Y chromosome partial microdeletions in different groups
|
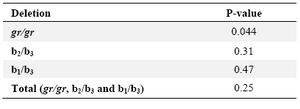
Table 5. Correlation of BMI with partial AZFc microdeletions of Fisher exact test
|
|